NEET MDS Lessons
Orthodontics
Tongue Thrust
Tongue thrust is characterized by the forward movement of the tongue tip between the teeth to meet the lower lip during swallowing and speech, resulting in an interdental position of the tongue (Tulley, 1969). This habit can lead to various dental and orthodontic issues, particularly malocclusions such as anterior open bite.
Etiology of Tongue Thrust
-
Retained Infantile Swallow:
- The tongue does not drop back as it should after the eruption of incisors, continuing to thrust forward during swallowing.
-
Upper Respiratory Tract Infection:
- Conditions such as mouth breathing and allergies can contribute to tongue thrusting behavior.
-
Neurological Disturbances:
- Issues such as hyposensitivity of the palate or disruption of sensory control and coordination during swallowing can lead to tongue thrust.
-
Feeding Practices:
- Bottle feeding is more likely to contribute to the development of tongue thrust compared to breastfeeding.
-
Induced by Other Oral Habits:
- Habits like thumb sucking or finger sucking can create malocclusions (e.g., anterior open bite), leading to the tongue protruding between the anterior teeth during swallowing.
-
Hereditary Factors:
- A family history of tongue thrusting or related oral habits may contribute to the development of the condition.
-
Tongue Size:
- Conditions such as macroglossia (enlarged tongue) can predispose individuals to tongue thrusting.
Clinical Features
Extraoral
- Lip Posture: Increased lip separation both at rest and during function.
- Mandibular Movement: The path of mandibular movement is upward and backward, with the tongue moving forward.
- Speech: Articulation problems, particularly with sounds such as /s/, /n/, /t/, /d/, /l/, /th/, /z/, and /v/.
- Facial Form: Increased anterior facial height may be observed.
Intraoral
- Tongue Posture: The tongue tip is lower at rest due to the presence of an anterior open bite.
- Malocclusion:
- Maxilla:
- Proclination of maxillary anterior teeth.
- Increased overjet.
- Maxillary constriction.
- Generalized spacing between teeth.
- Mandible:
- Retroclination of mandibular teeth.
- Maxilla:
Diagnosis
History
- Family History: Determine the swallow patterns of siblings and parents to check for hereditary factors.
- Medical History: Gather information regarding upper respiratory infections and sucking habits.
- Patient Motivation: Assess the patient�s overall abilities, interests, and motivation for treatment.
Examination
-
Swallowing Assessment:
- Normal Swallowing:
- Lips touch tightly.
- Mandible rises as teeth come together.
- Facial muscles show no marked contraction.
- Abnormal Swallowing:
- Teeth remain apart.
- Lips do not touch.
- Facial muscles show marked contraction.
- Normal Swallowing:
-
Inhibition Test:
- Lightly hold the lower lip with a thumb and finger while the patient is asked to swallow water.
- Normal Swallowing: The patient can swallow normally.
- Abnormal Swallowing: The swallow is inhibited, requiring strong mentalis and lip contraction for mandibular stabilization, leading to water spilling from the mouth.
Management
-
Behavioral Therapy:
- Awareness Training: Educate the patient about the habit and its effects on oral health.
- Positive Reinforcement: Encourage the patient to practice proper swallowing techniques and reward progress.
-
Myofunctional Therapy:
- Involves exercises to improve tongue posture and function, helping to retrain the muscles involved in swallowing and speech.
-
Orthodontic Treatment:
- If malocclusion is present, orthodontic intervention may be necessary to correct the dental alignment and occlusion.
- Appliances such as a palatal crib or tongue thrusting appliances can be used to discourage the habit.
-
Speech Therapy:
- If speech issues are present, working with a speech therapist can help address articulation problems and improve speech clarity.
-
Monitoring and Follow-Up:
- Regular follow-up appointments to monitor progress and make necessary adjustments to the treatment plan.
BONES OF THE SKULL
A) Bones of the cranial base:
A) Fontal (1)
B) Ethmoid (1)
C) Sphenoid (1)
D) Occipital (1)
B) Bones of the cranial vault:
1. Parietal (2)
2. Temporal (2)
C) Bones of the face:
Maxilla (2)
Mandible (1)
Nasal bone (2)
Lacrimal bone (2)
Zygomatic bone (2)
Palatine bone(2)
Infra nasal concha (2)
FUSION BETWEEN BONES
1. Syndesmosis: Membranous or ligamentus eg. Sutural point.
2. Synostosis: Bony union eg. symphysis menti.
3. Synchondrosis: Cartilaginous eg. sphenoccipital, spheno-ethmoidal.
GROWTH OF THE SKULL:
A) Cranium: 1. Base 2. Vault
B) Face: 1. Upper face 2.Lower face
CRANIAL BASE:
Cranial base grows at different cartilaginous suture. The cranial base may be divided into 3 areas.
1. The posterior part which extends from the occiput to the salatercica. The most important growth site spheno-occipital synchondrosis is situated here. It is active throughout the growing period and does not close until early adult life.
2. The middle portion extends from sella to foramen cecum and the sutural growth spheno-ethmoidal synchondrosis is situated here. The exact time of closing is not known but probably at the age of 7 years.
3. The anterior part is from foramen cecum and grows by surface deposition of bone in the frontal region and simultaneous development of frontal sinus.
CRANIAL VAULT:
The cranial vault grows as the brain grows. It is accelerated at infant. The growth is complete by 90% by the end of 5th year. At birth the sutures are wide sufficiently and become approximated during the 1st 2 years of life.
The development and extension of frontal sinus takes place particularly at the age of puberty and there is deposition of bone on the surfaces of cranial bone.
Functional Matrix Hypothesis is a concept in orthodontics and craniofacial biology that explains how the growth and development of the craniofacial complex (including the skull, face, and dental structures) are influenced by functional demands and environmental factors rather than solely by genetic factors. This hypothesis was proposed by Dr. Robert A. K. McNamara and is based on the idea that the functional matrices�such as muscles, soft tissues, and functional activities (like chewing and speaking)�play a crucial role in shaping the skeletal structures.
Concepts of the Functional Matrix Hypothesis
-
Functional Matrices:
- The hypothesis posits that the growth of the craniofacial skeleton
is guided by the functional matrices surrounding it. These matrices
include:
- Muscles: The muscles of mastication, facial expression, and other soft tissues exert forces on the bones, influencing their growth and development.
- Soft Tissues: The presence and tension of soft tissues, such as the lips, cheeks, and tongue, can affect the position and growth of the underlying skeletal structures.
- Functional Activities: Activities such as chewing, swallowing, and speaking create functional demands that influence the growth patterns of the craniofacial complex.
- The hypothesis posits that the growth of the craniofacial skeleton
is guided by the functional matrices surrounding it. These matrices
include:
-
Growth and Development:
- According to the Functional Matrix Hypothesis, the growth of the craniofacial skeleton is not a direct result of genetic programming but is instead a response to the functional demands placed on it. This means that changes in function can lead to changes in growth patterns.
- For example, if a child has a habit of mouth breathing, the lack of proper nasal function can lead to altered growth of the maxilla and mandible, resulting in malocclusion or other dental issues.
-
Orthodontic Implications:
- The Functional Matrix Hypothesis has significant implications for
orthodontic treatment and craniofacial orthopedics. It suggests that:
- Functional Appliances: Orthodontic appliances that modify function (such as functional appliances) can be used to influence the growth of the jaws and improve occlusion.
- Early Intervention: Early orthodontic intervention may be beneficial in guiding the growth of the craniofacial complex, especially in children, to prevent or correct malocclusions.
- Holistic Approach: Treatment should consider not only the teeth and jaws but also the surrounding soft tissues and functional activities.
- The Functional Matrix Hypothesis has significant implications for
orthodontic treatment and craniofacial orthopedics. It suggests that:
-
Clinical Applications:
- The Functional Matrix Hypothesis encourages clinicians to assess the functional aspects of a patient's oral and facial structures when planning treatment. This includes evaluating muscle function, soft tissue relationships, and the impact of habits (such as thumb sucking or mouth breathing) on growth and development.
Thumb Sucking
According to Gellin, thumb sucking is defined as �the placement of the thumb or one or more fingers in varying depth into the mouth.� This behavior is common in infants and young children, serving as a self-soothing mechanism. However, prolonged thumb sucking can lead to various dental and orthodontic issues.
Diagnosis of Thumb Sucking
1. History
- Psychological Component: Assess any underlying psychological factors that may contribute to the habit, such as anxiety or stress.
- Frequency, Intensity, and Duration: Gather information on how often the child engages in thumb sucking, how intense the habit is, and how long it has been occurring.
- Feeding Patterns: Inquire about the child�s feeding habits, including breastfeeding or bottle-feeding, as these can influence thumb sucking behavior.
- Parental Care: Evaluate the parenting style and care provided to the child, as this can impact the development of habits.
- Other Habits: Assess for the presence of other oral habits, such as pacifier use or nail-biting, which may coexist with thumb sucking.
2. Extraoral Examination
- Digits:
- Appearance: The fingers may appear reddened, exceptionally clean, chapped, or exhibit short fingernails (often referred to as "dishpan thumb").
- Calluses: Fibrous, roughened calluses may be present on the superior aspect of the finger.
- Lips:
- Upper Lip: May appear short and hypotonic (reduced muscle tone).
- Lower Lip: Often hyperactive, showing increased movement or tension.
- Facial Form Analysis:
- Mandibular Retrusion: Check for any signs of the lower jaw being positioned further back than normal.
- Maxillary Protrusion: Assess for any forward positioning of the upper jaw.
- High Mandibular Plane Angle: Evaluate the angle of the mandible, which may be increased due to the habit.
3. Intraoral Examination
-
Clinical Features:
- Intraoral:
- Labial Flaring: Maxillary anterior teeth may show labial flaring due to the pressure from thumb sucking.
- Lingual Collapse: Mandibular anterior teeth may exhibit lingual collapse.
- Increased Overjet: The distance between the upper and lower incisors may be increased.
- Hypotonic Upper Lip: The upper lip may show reduced muscle tone.
- Hyperactive Lower Lip: The lower lip may be more active, compensating for the upper lip.
- Tongue Position: The tongue may be placed inferiorly, leading to a posterior crossbite due to maxillary arch contraction.
- High Palatal Vault: The shape of the palate may be altered, resulting in a high palatal vault.
- Intraoral:
-
Extraoral:
- Fungal Infection: There may be signs of fungal infection on the thumb due to prolonged moisture exposure.
- Thumb Nail Appearance: The thumb nail may exhibit a dishpan appearance, indicating frequent moisture exposure and potential damage.
Management of Thumb Sucking
1. Reminder Therapy
- Description: This involves using reminders to help the child become aware of their thumb sucking habit. Parents and caregivers can gently remind the child to stop when they notice them sucking their thumb. Positive reinforcement for not engaging in the habit can also be effective.
2. Mechanotherapy
- Description: This approach involves using mechanical
devices or appliances to discourage thumb sucking. Some options include:
- Thumb Guards: These are devices that fit over the thumb to prevent sucking.
- Palatal Crib: A fixed appliance that can be placed in the mouth to make thumb sucking uncomfortable or difficult.
- Behavioral Appliances: Appliances that create discomfort when the child attempts to suck their thumb, thereby discouraging the habit.
Types of Fixed Orthodontic Appliances
-
Braces:
- Traditional Metal Braces: Composed of metal brackets bonded to the teeth, connected by archwires. They are the most common type of fixed appliance.
- Ceramic Braces: Similar to metal braces but made of tooth-colored or clear materials, making them less visible.
- Lingual Braces: Brackets are placed on the inner surface of the teeth, making them invisible from the outside.
-
Self-Ligating Braces:
- These braces use a specialized clip mechanism to hold the archwire in place, eliminating the need for elastic or metal ligatures. They can reduce friction and may allow for faster tooth movement.
-
Space Maintainers:
- Fixed appliances used to hold space for permanent teeth when primary teeth are lost prematurely. They are typically bonded to adjacent teeth.
-
Temporary Anchorage Devices (TADs):
- Small screws or plates that are temporarily placed in the bone to provide additional anchorage for tooth movement. They help in achieving specific movements without unwanted tooth movement.
-
Palatal Expanders:
- Fixed appliances used to widen the upper jaw (maxilla) by applying pressure to the molars. They are often used in growing patients to correct crossbites or narrow arches.
Components of Fixed Orthodontic Appliances
- Brackets: Small metal or ceramic attachments bonded to the teeth. They hold the archwire in place and guide tooth movement.
- Archwires: Thin metal wires that connect the brackets and apply pressure to the teeth. They come in various materials and sizes, and their shape can be adjusted to achieve desired movements.
- Ligatures: Small elastic or metal ties that hold the archwire to the brackets. In self-ligating braces, ligatures are not needed.
- Bands: Metal rings that are cemented to the molars to provide anchorage for the appliance. They may have attachments for brackets or other components.
- Hooks and Accessories: Additional components that can be attached to brackets or bands to facilitate the use of elastics or other auxiliary devices.
Indications for Use
- Correction of Malocclusions: Fixed appliances are commonly used to treat various types of malocclusions, including crowding, spacing, overbites, underbites, and crossbites.
- Tooth Movement: They are effective for moving teeth into desired positions, including tipping, bodily movement, and rotation.
- Retention: Fixed retainers may be used after active treatment to maintain the position of teeth.
- Jaw Relationship Modification: Fixed appliances can help in correcting skeletal discrepancies and improving the relationship between the upper and lower jaws.
Advantages of Fixed Orthodontic Appliances
- Continuous Force Application: Fixed appliances provide a constant force on the teeth, allowing for more predictable and efficient tooth movement.
- Effective for Complex Cases: They are suitable for treating a wide range of orthodontic issues, including severe malocclusions that may not be effectively treated with removable appliances.
- Patient Compliance: Since they are fixed, there is no reliance on patient compliance for wearing the appliance, which can lead to more consistent treatment outcomes.
- Variety of Options: Patients can choose from various types of braces (metal, ceramic, lingual) based on their aesthetic preferences.
Disadvantages of Fixed Orthodontic Appliances
- Oral Hygiene Challenges: Fixed appliances can make it more difficult to maintain oral hygiene, increasing the risk of plaque accumulation, cavities, and gum disease.
- Discomfort: Patients may experience discomfort or soreness after adjustments, especially in the initial stages of treatment.
- Dietary Restrictions: Certain foods (hard, sticky, or chewy) may need to be avoided to prevent damage to the appliances.
- Duration of Treatment: Treatment with fixed appliances can take several months to years, depending on the complexity of the case.
Growth is the increase in size It may also be defined as the normal� change in the amount of living substance. eg. Growth is the quantitative aspect and measures in units of increase per unit of time.
Development
It is the progress towards maturity (Todd). Development may be defined as natural sequential series of events between fertilization of ovum and adult stage.
Maturation
It is a period of stabilization brought by growth and development.
CEPHALOCAUDAL GRADIENT OF GROWTH
This simply means that there is an axis of increased growth extending from the head towards feet. At about 3rd month of intrauterine life the head takes up about 50% of total body length. At this stage cranium is larger relative to face. In contrast the limbs are underdeveloped.�
By the time of birth limbs and trunk have grown faster than head and the entire proportion of the body to the head has increased. These processes of growth continue till adult.��
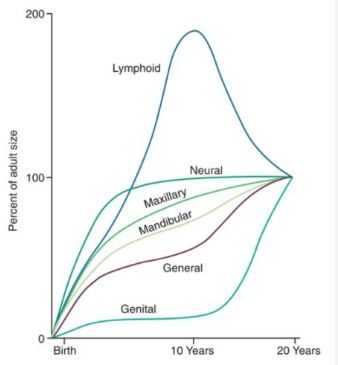
SCAMMON�S CURVE
In normal growth pattern all the tissue system of the body do not growth at the same rate. Scammon�s curve for growth shows 4 major tissue system of the body;
� Neural
� Lymphoid�
� General: Bone, viscera, muscle.
� Genital
The graph indicates the growth of the neural tissue is complete by 6-7 year of age. General body tissue show an �S� shaped curve with showing of rate during childhood and acceleration at puberty. Lymphoid tissues proliferate to its maximum in late childhood and undergo involution. At the same time growth of the genital tissue accelerate rapidly.�
�
Angle�s Classification of Malocclusion
Malocclusion refers to the misalignment or incorrect relationship between the teeth of the two dental arches when they come into contact as the jaws close. Understanding occlusion is essential for diagnosing and treating orthodontic issues.
Definitions
- Occlusion: The contact between the teeth in the mandibular arch and those in the maxillary arch during functional relations (Wheeler�s definition).
- Malocclusion: A condition characterized by a deflection from the normal relation of the teeth to other teeth in the same arch and/or to teeth in the opposing arch (Gardiner, White & Leighton).
Importance of Classification
Classifying malocclusion serves several purposes:
- Grouping of Orthodontic Problems: Helps in identifying and categorizing various orthodontic issues.
- Location of Problems: Aids in pinpointing specific areas that require treatment.
- Diagnosis and Treatment Planning: Facilitates the development of effective treatment strategies.
- Self-Communication: Provides a standardized language for orthodontists to discuss cases.
- Documentation: Useful for recording and tracking orthodontic problems.
- Epidemiological Studies: Assists in research and studies related to malocclusion prevalence.
- Assessment of Treatment Effects: Evaluates the effectiveness of orthodontic appliances.
Normal Occlusion
Molar Relationship
According to Angle, normal occlusion is defined by the relationship of the mesiobuccal cusp of the maxillary first molar aligning with the buccal groove of the mandibular first molar.
Angle�s Classification of Malocclusion
Edward Angle, known as the father of modern orthodontics, first published his classification in 1899. The classification is based on the relationship of the mesiobuccal cusp of the maxillary first molar to the buccal groove of the mandibular first molar. It is divided into three classes:
Class I Malocclusion (Neutrocclusion)
- Definition: Normal molar relationship is present, but there may be crowding, misalignment, rotations, cross-bites, and other irregularities.
- Characteristics:
- Molar relationship is normal.
- Teeth may be crowded or rotated.
- Other alignment irregularities may be present.
Class II Malocclusion (Distocclusion)
- Definition: The lower molar is positioned distal to the upper molar.
- Characteristics:
- Often results in a retrognathic facial profile.
- Increased overjet and overbite.
- The mesiobuccal cusp of the maxillary first molar occludes anterior to the buccal groove of the mandibular first molar.
Subdivisions of Class II Malocclusion:
- Class II Division 1:
- Class II molars with normally inclined or proclined maxillary central incisors.
- Class II Division 2:
- Class II molars with retroclined maxillary central incisors.
Class III Malocclusion (Mesiocclusion)
- Definition: The lower molar is positioned mesial to the upper molar.
- Characteristics:
- Often results in a prognathic facial profile.
- Anterior crossbite and negative overjet (underbite).
- The mesiobuccal cusp of the upper first molar falls posterior to the buccal groove of the lower first molar.
Advantages of Angle�s Classification
- Comprehensive: It is the first comprehensive classification and is widely accepted in the field of orthodontics.
- Simplicity: The classification is straightforward and easy to use.
- Popularity: It is the most popular classification system among orthodontists.
- Effective Communication: Facilitates clear communication regarding malocclusion.
Disadvantages of Angle�s Classification
- Limited Plane Consideration: It primarily considers malocclusion in the anteroposterior plane, neglecting transverse and vertical dimensions.
- Fixed Reference Point: The first molar is considered a fixed point, which may not be applicable in all cases.
- Not Applicable for Deciduous Dentition: The classification does not effectively address malocclusion in children with primary teeth.
- Lack of Distinction: It does not differentiate between skeletal and dental malocclusion.