NEET MDS Lessons
Orthodontics
Growth is the increase in size It may also be defined as the normal� change in the amount of living substance. eg. Growth is the quantitative aspect and measures in units of increase per unit of time.
Development
It is the progress towards maturity (Todd). Development may be defined as natural sequential series of events between fertilization of ovum and adult stage.
Maturation
It is a period of stabilization brought by growth and development.
CEPHALOCAUDAL GRADIENT OF GROWTH
This simply means that there is an axis of increased growth extending from the head towards feet. At about 3rd month of intrauterine life the head takes up about 50% of total body length. At this stage cranium is larger relative to face. In contrast the limbs are underdeveloped.�
By the time of birth limbs and trunk have grown faster than head and the entire proportion of the body to the head has increased. These processes of growth continue till adult.��
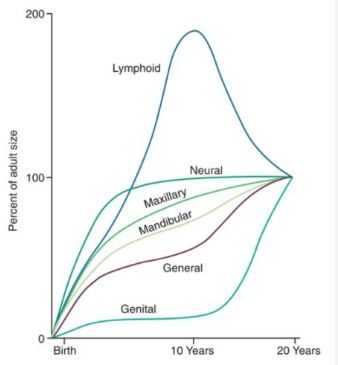
SCAMMON�S CURVE
In normal growth pattern all the tissue system of the body do not growth at the same rate. Scammon�s curve for growth shows 4 major tissue system of the body;
� Neural
� Lymphoid�
� General: Bone, viscera, muscle.
� Genital
The graph indicates the growth of the neural tissue is complete by 6-7 year of age. General body tissue show an �S� shaped curve with showing of rate during childhood and acceleration at puberty. Lymphoid tissues proliferate to its maximum in late childhood and undergo involution. At the same time growth of the genital tissue accelerate rapidly.�
�
Relapse
Definition: Relapse refers to the tendency of teeth to return to their original positions after orthodontic treatment. This can occur due to various factors, including the natural elasticity of the periodontal ligament, muscle forces, and the influence of oral habits.
Causes of Relapse
- Elasticity of the Periodontal Ligament: After orthodontic treatment, the periodontal ligament may still have a tendency to revert to its original state, leading to tooth movement.
- Muscle Forces: The forces exerted by the lips, cheeks, and tongue can influence tooth positions, especially if these forces are not balanced.
- Growth and Development: In growing patients, changes in jaw size and shape can lead to shifts in tooth positions.
- Non-Compliance with Retainers: Failure to wear retainers as prescribed can significantly increase the risk of relapse.
Prevention of Relapse
- Consistent Retainer Use: Adhering to the retainer regimen as prescribed by the orthodontist is crucial for maintaining tooth positions.
- Regular Follow-Up Visits: Periodic check-ups with the orthodontist can help monitor tooth positions and address any concerns early.
- Patient Education: Educating patients about the importance of retention and the potential for relapse can improve compliance with retainer wear.
Angle's Classification of Malocclusion
Developed by Dr. Edward Angle in the early 20th century, this classification is based on the relationship of the first molars and the canines. It is divided into three main classes:
Class I Malocclusion (Normal Occlusion)
- Description: The first molars are in a normal relationship, with the mesiobuccal cusp of the maxillary first molar fitting into the buccal groove of the mandibular first molar. The canines also have a normal relationship.
- Characteristics:
- The dental arches are aligned.
- There may be crowding, spacing, or other dental irregularities, but the overall molar relationship is normal.
Class II Malocclusion (Distocclusion)
- Description: The first molars are positioned such that the mesiobuccal cusp of the maxillary first molar is positioned more than one cusp width ahead of the buccal groove of the mandibular first molar.
- Subdivisions:
- Class II Division 1: Characterized by protruded maxillary incisors and a deep overbite.
- Class II Division 2: Characterized by retroclined maxillary incisors and a deep overbite, often with a normal or reduced overjet.
- Characteristics: This class often results in an overbite and can lead to aesthetic concerns.
Class III Malocclusion (Mesioocclusion)
- Description: The first molars are positioned such that the mesiobuccal cusp of the maxillary first molar is positioned more than one cusp width behind the buccal groove of the mandibular first molar.
- Characteristics:
- This class is often associated with an underbite, where the lower teeth are positioned more forward than the upper teeth.
- It can lead to functional issues and aesthetic concerns.
2. Skeletal Classification
In addition to Angle's classification, malocclusion can also be classified based on skeletal relationships, which consider the position of the maxilla and mandible in relation to each other. This classification is particularly useful in assessing the underlying skeletal discrepancies that may contribute to malocclusion.
Class I Skeletal Relationship
- Description: The maxilla and mandible are in a normal relationship, similar to Class I malocclusion in Angle's classification.
- Characteristics: The skeletal bases are well-aligned, but there may still be dental irregularities.
Class II Skeletal Relationship
- Description: The mandible is positioned further back relative to the maxilla, similar to Class II malocclusion.
- Characteristics: This can be due to a retruded mandible or an overdeveloped maxilla.
Class III Skeletal Relationship
- Description: The mandible is positioned further forward relative to the maxilla, similar to Class III malocclusion.
- Characteristics: This can be due to a protruded mandible or a retruded maxilla.
3. Other Classifications
In addition to Angle's and skeletal classifications, malocclusion can also be described based on specific characteristics:
-
Overbite: The vertical overlap of the upper incisors over the lower incisors. It can be classified as:
- Normal Overbite: Approximately 1-2 mm of overlap.
- Deep Overbite: Excessive overlap, which can lead to impaction of the lower incisors.
- Open Bite: Lack of vertical overlap, where the upper and lower incisors do not touch.
-
Overjet: The horizontal distance between the labioincisal edge of the upper incisors and the linguoincisal edge of the lower incisors. It can be classified as:
- Normal Overjet: Approximately 2-4 mm.
- Increased Overjet: Greater than 4 mm, often associated with Class II malocclusion.
- Decreased Overjet: Less than 2 mm, often associated with Class III malocclusion.
-
Crossbite: A condition where one or more of the upper teeth bite on the inside of the lower teeth. It can be:
- Anterior Crossbite: Involves the front teeth.
- Posterior Crossbite: Involves the back teeth.
Thumb Sucking
According to Gellin, thumb sucking is defined as �the placement of the thumb or one or more fingers in varying depth into the mouth.� This behavior is common in infants and young children, serving as a self-soothing mechanism. However, prolonged thumb sucking can lead to various dental and orthodontic issues.
Diagnosis of Thumb Sucking
1. History
- Psychological Component: Assess any underlying psychological factors that may contribute to the habit, such as anxiety or stress.
- Frequency, Intensity, and Duration: Gather information on how often the child engages in thumb sucking, how intense the habit is, and how long it has been occurring.
- Feeding Patterns: Inquire about the child�s feeding habits, including breastfeeding or bottle-feeding, as these can influence thumb sucking behavior.
- Parental Care: Evaluate the parenting style and care provided to the child, as this can impact the development of habits.
- Other Habits: Assess for the presence of other oral habits, such as pacifier use or nail-biting, which may coexist with thumb sucking.
2. Extraoral Examination
- Digits:
- Appearance: The fingers may appear reddened, exceptionally clean, chapped, or exhibit short fingernails (often referred to as "dishpan thumb").
- Calluses: Fibrous, roughened calluses may be present on the superior aspect of the finger.
- Lips:
- Upper Lip: May appear short and hypotonic (reduced muscle tone).
- Lower Lip: Often hyperactive, showing increased movement or tension.
- Facial Form Analysis:
- Mandibular Retrusion: Check for any signs of the lower jaw being positioned further back than normal.
- Maxillary Protrusion: Assess for any forward positioning of the upper jaw.
- High Mandibular Plane Angle: Evaluate the angle of the mandible, which may be increased due to the habit.
3. Intraoral Examination
-
Clinical Features:
- Intraoral:
- Labial Flaring: Maxillary anterior teeth may show labial flaring due to the pressure from thumb sucking.
- Lingual Collapse: Mandibular anterior teeth may exhibit lingual collapse.
- Increased Overjet: The distance between the upper and lower incisors may be increased.
- Hypotonic Upper Lip: The upper lip may show reduced muscle tone.
- Hyperactive Lower Lip: The lower lip may be more active, compensating for the upper lip.
- Tongue Position: The tongue may be placed inferiorly, leading to a posterior crossbite due to maxillary arch contraction.
- High Palatal Vault: The shape of the palate may be altered, resulting in a high palatal vault.
- Intraoral:
-
Extraoral:
- Fungal Infection: There may be signs of fungal infection on the thumb due to prolonged moisture exposure.
- Thumb Nail Appearance: The thumb nail may exhibit a dishpan appearance, indicating frequent moisture exposure and potential damage.
Management of Thumb Sucking
1. Reminder Therapy
- Description: This involves using reminders to help the child become aware of their thumb sucking habit. Parents and caregivers can gently remind the child to stop when they notice them sucking their thumb. Positive reinforcement for not engaging in the habit can also be effective.
2. Mechanotherapy
- Description: This approach involves using mechanical
devices or appliances to discourage thumb sucking. Some options include:
- Thumb Guards: These are devices that fit over the thumb to prevent sucking.
- Palatal Crib: A fixed appliance that can be placed in the mouth to make thumb sucking uncomfortable or difficult.
- Behavioral Appliances: Appliances that create discomfort when the child attempts to suck their thumb, thereby discouraging the habit.
Catalan's Appliance
Catalan's appliance, also known as the Catalan appliance or lower inclined bite plane, is an orthodontic device primarily used to correct anterior crossbites and manage dental arch relationships. It is particularly effective in growing children and adolescents, as it helps to guide the development of the dental arches and improve occlusion.
Indications for Use
-
Anterior Crossbite:
- The primary indication for Catalan's appliance is to correct anterior crossbites, where the upper front teeth are positioned behind the lower front teeth when the jaws are closed.
-
Space Management:
- It can be used to create space in the dental arch, especially when there is crowding or insufficient space for the eruption of permanent teeth.
-
Guiding Eruption:
- The appliance helps guide the eruption of the permanent teeth into a more favorable position, promoting proper alignment.
-
Facilitating Growth:
- It can assist in the growth of the maxilla and mandible, helping to achieve a more balanced facial profile.
Design and Features
-
Components:
- The Catalan's appliance typically consists of:
- Acrylic Base: A custom-fitted acrylic base that covers the lower anterior teeth.
- Inclined Plane: An inclined plane is incorporated into the appliance, which helps to reposition the anterior teeth by providing a surface for the teeth to occlude against.
- Retention Mechanism: The appliance is retained in the mouth using clasps or other anchorage methods to ensure stability during treatment.
- The Catalan's appliance typically consists of:
-
Customization:
- The appliance is custom-made for each patient based on their specific dental anatomy and treatment needs. This ensures a proper fit and effective function.
Mechanism of Action
-
Correction of Crossbite:
- The inclined plane of the Catalan's appliance exerts forces on the anterior teeth, encouraging them to move into a more favorable position. This helps to correct the crossbite by allowing the maxillary incisors to move forward relative to the mandibular incisors.
-
Space Creation:
- By repositioning the anterior teeth, the appliance can create additional space in the dental arch, facilitating the eruption of permanent teeth and improving overall alignment.
-
Guiding Eruption:
- The appliance helps guide the eruption of the permanent teeth by maintaining proper arch form and preventing unwanted movements of the teeth.
Frankel appliance is a functional orthodontic device designed to guide facial growth and correct malocclusions. There are four main types: Frankel I (for Class I and Class II Division 1 malocclusions), Frankel II (for Class II Division 2), Frankel III (for Class III malocclusions), and Frankel IV (for specific cases requiring unique adjustments). Each type addresses different dental and skeletal relationships.
The Frankel appliance is a removable orthodontic device that plays a crucial role in the treatment of various malocclusions. It is designed to influence the growth of the jaw and dental arches by modifying muscle function and promoting proper alignment of teeth.
Types of Frankel Appliances
-
Frankel I:
- Indications: Primarily used for Class I and Class II Division 1 malocclusions.
- Function: Helps in correcting overjet and improving dental alignment.
-
Frankel II:
- Indications: Specifically designed for Class II Division 2 malocclusions.
- Function: Aims to reposition the maxilla and improve the relationship between the upper and lower teeth.
-
Frankel III:
- Indications: Used for Class III malocclusions.
- Function: Encourages forward positioning of the maxilla and helps in correcting the skeletal relationship.
-
Frankel IV:
- Indications: Suitable for open bites and bimaxillary protrusions.
- Function: Focuses on creating space and improving the occlusion by addressing specific dental and skeletal issues.
Key Features of Frankel Appliances
-
Myofunctional Design: The appliance is designed to utilize the forces generated by muscle function to guide the growth of the dental arches.
-
Removable: Patients can take the appliance out for cleaning and during meals, which enhances comfort and hygiene.
-
Custom Fit: Each appliance is tailored to the individual patient's dental anatomy, ensuring effective treatment.
Treatment Goals
-
Facial Balance: The primary goal of using a Frankel appliance is to achieve facial harmony and balance by correcting malocclusions.
-
Functional Improvement: It promotes the establishment of normal muscle function, which is essential for long-term dental health.
-
Arch Development: The appliance aids in the development of the dental arches, providing adequate space for the eruption of permanent teeth.
Anchorage in orthodontics refers to the resistance that the anchorage area offers to unwanted tooth movements during orthodontic treatment. Proper understanding and application of anchorage principles are crucial for achieving desired tooth movements while minimizing undesirable effects on adjacent teeth.
Classification of Anchorage
1. According to Manner of Force Application
-
Simple Anchorage:
- Achieved by engaging a greater number of teeth than those being moved within the same dental arch.
- The combined root surface area of the anchorage unit must be at least double that of the teeth to be moved.
-
Stationary Anchorage:
- Defined as dental anchorage where the application of force tends to displace the anchorage unit bodily in the direction of the force.
- Provides greater resistance compared to anchorage that only resists tipping forces.
-
Reciprocal Anchorage:
- Refers to the resistance offered by two malposed units when equal and opposite forces are applied, moving each unit towards a more normal occlusion.
- Examples:
- Closure of a midline diastema by moving the two central incisors towards each other.
- Use of crossbite elastics and dental arch expansions.
2. According to Jaws Involved
- Intra-maxillary Anchorage:
- All units offering resistance are situated within the same jaw.
- Intermaxillary Anchorage:
- Resistance units in one jaw are used to effect tooth movement in the opposing jaw.
- Also known as Baker's anchorage.
- Examples:
- Class II elastic traction.
- Class III elastic traction.
3. According to Site
-
Intraoral Anchorage:
- Both the teeth to be moved and the anchorage areas are located within the oral cavity.
- Anatomic units include teeth, palate, and lingual alveolar bone of the mandible.
-
Extraoral Anchorage:
- Resistance units are situated outside the oral cavity.
- Anatomic units include the occiput, back of the neck, cranium, and face.
- Examples:
- Headgear.
- Facemask.
-
Muscular Anchorage:
- Utilizes forces generated by muscles to aid in tooth movement.
- Example: Lip bumper to distalize molars.
4. According to Number of Anchorage Units
-
Single or Primary Anchorage:
- A single tooth with greater alveolar support is used to move another tooth with lesser support.
-
Compound Anchorage:
- Involves more than one tooth providing resistance to move teeth with lesser support.
-
Multiple or Reinforced Anchorage:
- Utilizes more than one type of resistance unit.
- Examples:
- Extraoral forces to augment anchorage.
- Upper anterior inclined plane.
- Transpalatal arch.